About the East Kent CTS Care Pathway
The care pathway was introduced in April 2004, since then increasing numbers of patients have been sent along this route by their general practitioners. Prior to the introduction of this pathway the commonest sequence of events for a patient presenting to their GP with symptoms suggestive of CTS was a referral to orthopaedic outpatients. From there most patients would be referred for neurophysiological testing, entailing a second visit to hospital, and would then be reviewed in a further orthopaedic outpatient clinic before being placed on a surgery waiting list.
The new pathway allows a general practitioner who suspects CTS to refer the patient directly for a visit to the neurophysiology department in Canterbury where tests can be performed and a plan for treatment made all in one visit. Much of the treatment is then carried out back in primary care. The CTS clinic is operated by a team comprising administrative staff, a group of clinical scientists who perform the nerve conduction studies and three individuals with a special interest in carpal tunnel syndrome:
Dr Jeremy Bland - Consultant in Clinical Neurophysiology, in overall charge
Mr Michael Nicholas - Surgical Care practitioner, who carries out injections and many operations for CTS
Ms Emma Kaile - CTS practitioner, a new appointment who will be learning to run the clinic independently in time
The numbers of referrals to the new pathway by calendar month from April 2004 to March 2011 are shown here:
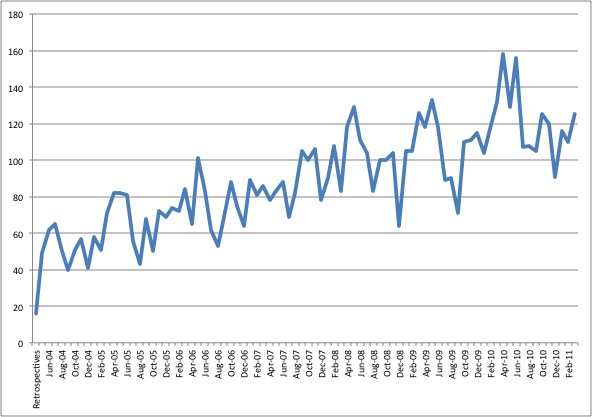
At the same time that the number of referrals to the scheme has been increasing it has also represented an increasing proportion of all general practice requests for nerve conduction studies for CTS, rising from about 50% at the outset to about 90% now:
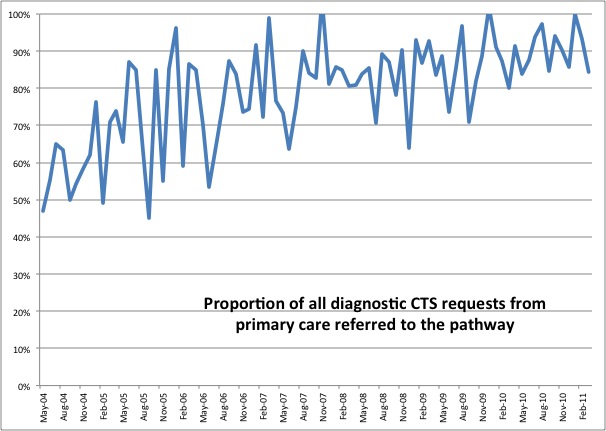
In the new pathway, patients start with a visit to the neurophysiology department in Canterbury which is combined with a treatment planning consultation at the same visit if the diagnosis is confirmed which it currently is in two thirds of cases. Most treatment is then carried out in primary care though we are carrying out an increasing number of local steroid injections at the initial visit too. The breakdown of subsequent choice of initial treatment after that consultation is as follows:
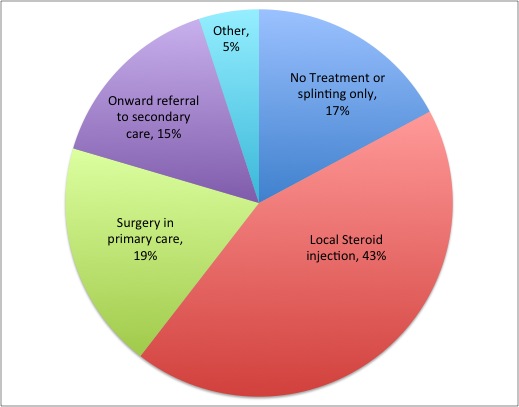
Patients are generally referred on to other secondary care clinics either because they have complex problems requiring the assistance of a specialist hand surgeon, rheumatologist or neurologist, or have to have surgery in hospital because of medical risk factors for surgery in primary care such as anticoagulation or unstable angina or diabetes. A few individuals decide to continue their care in the private sector.
Our basic recommendations regarding treatment are based on our locally collected data on the outcome of surgical treatment. As patients with grade 1 and 2 CTS seem to do less well with surgery we tend to prefer non-surgical care for these, at least initially, whereas for grade 4 and 5 it appears that going straight to surgery is the better option. The local policy also stipulates that grade 6 cases will all be sent for an opinion from a specialist hand surgeon as treating these cases can be problematic. It should be noted that it is not possible to work out what grade your CTS is without carrying out full nerve conduction studies. The results provided by small handheld nerve conduction machines are not detailed enough to permit grading and it is not possible to tell what grade a hand is from the severity of the symptoms nor from examination, except for grade 6 - by which time it is too late for the most effective treatment.
Although the above is our 'default' plan of action many individual circumstances can modify this and the actual choice of initial treatment chosen by patients with each grade of CTS is shown below:
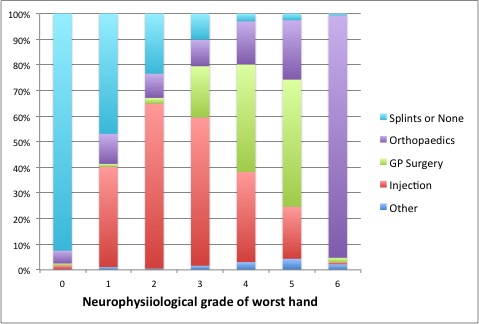
Note that the local policy does not make a firm recommendation for grade 3 CTS and the decision for these is mainly influenced by patient preference. Note also that some patients with severe CTS choose not to undergo surgery. How many patients present in each severity grade?
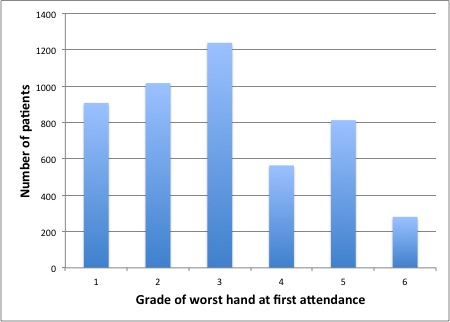
Grade three is therefore the commonest and many patients are faced with the dilemma of how to treat it.
In the current economic climate where much is heard about NHS cuts it is worth noting that the basic treatment recommendations here are based on the clinical outcomes of surgical treatment, irrespective of cost of the different treatments. We are however interested in health economics also and although we do not make treatment recommendations based upon cost we think it important for both patients and doctors to understand the costs of treatment and for managers and policy makers to appreciate the overall societal costs of CTS.
The impact of changes to the NHS introduced in April 2013
The arrangements described above were developed cooperatively between the neurophysiology service, hand surgeons, hand therapists, rheumatologists, general practitioners, and health service managers in the primary and secondary sectors in 2003-4. At that time the primary care managers were the 'East Kent Primary Care Trust' or PCT which had responsibility for spending the local health budget to buy care for the East Kent population. Following the changes introduced by the current government in April 2013 the one PCT which performed this 'purchasing' function for the whole East Kent area has been replaced with four geographically based 'Clinical Commissioning Groups' or CCGs, each one responsible for one part of what used to be the area covered by the East Kent PCT.
The four new CCGs are independently considering how best to deploy their available funds to purchase care for their population. At present they are taking different approaches to the existing CTS care pathway so that the treatment of individual cases can now differ depending on where the patient lives
Canterbury and Coastal CCG
Arrangements have been made for splints for carpal tunnel syndrome to be provided from GP practices and GPs in this area are encouraged to direct their patients to this website for information. For patients whose symptoms do not resolve completely with a few weeks of splinting, GPs in this CCG area can still refer to the Canterbury CTS clinic and from that point onwards arranegments continue as before - but see the note below regarding bookings for surgery in primary care.
South Kent Coast CCG
As for Canterbury and Coastal - GP practices have been provided with supplies of splints for CTS but referral to the CTS care pathway is then an option for GPs/patients in this area.
Ashford CCG
Ashford proposed more substantial changes to the management of CTS in a laudable attempt to provide care for CTS closer to patients homes. An alternative provider of a CTS service was commissioned - a clinic held at St Stephen's Health Centre in Ashford but after 2-3 years this was discontinued and Ashford patients are once again being referred to Canterbury for testing and arrangement of treatment. A new GP surgery arrangement is available to us in Ashford however and we can therefore offer patients some more local surgery appointments in Ashford at Willesborough Health Centre.
Thanet CCG
Thanet have taken a different approach to the provision of splinting. Recognising the logistic difficulty of keeping supplies of right and left sided splints in a variety of sizes available in every practice they have suggested that patients should purchase their own splints as an initial treatment for suspected CTS. They have also recommended, through a website that provides guidance for Thanet GPs on local resources (Where to Refer in Thanet - this currently seems to be offline), that patients should be directed to this website for information. Thanet GPs also remain able to refer patients to the specialist CTS clinic in Canterbury.
Booking of appointments for surgery in primary care
In the past, I have been able to agree a date and time for surgery in primary care with patients at the time of consultation with me and we have been able to arrange changes to such appointments and the filling of last minute cancellations by direct communication between the patient and the CTS clinic. Ashford CCG host the more general booking services for all of the minor surgery which is performed in primary care and now require that all bookings for carpal tunnel surgery (in primary care, not in hospital) are made through their administrative office in Ashford - on grounds of 'improved patient choice'. At present therefore I am afraid that we have to ask even patients from Margate to telephone the administrators in Ashford to confirm their choice of GP surgeon when opting for carpal tunnel surgery in primary care.
If you are unsure which CCG your GP practice belongs to - you can check at the websites of the individual CCGs
Canterbury and Coastal CCG website
The future of the East Kent CTS care pathway
We are currently working on a proposal for an improved version of the existing care pathway which will be acceptable to all four CCGs and which will retain uniform high quality treatment across the entire area. I would appreciate hearing any patient views which might help us to decide what changes should be made and postings on the subject are welcome in the website forums.
Revision date - 28th February 2019